Immunosuppressant Risk Assessment Tool
Your Personalized Risk Assessment
For years, doctors told patients with a history of cancer to wait at least five years before starting immunosuppressants. The fear was simple: if your immune system is turned down, it might not catch cancer coming back. But that advice? It was based on guesswork, not hard data. Today, we know better.
Why the old rule didn’t hold up
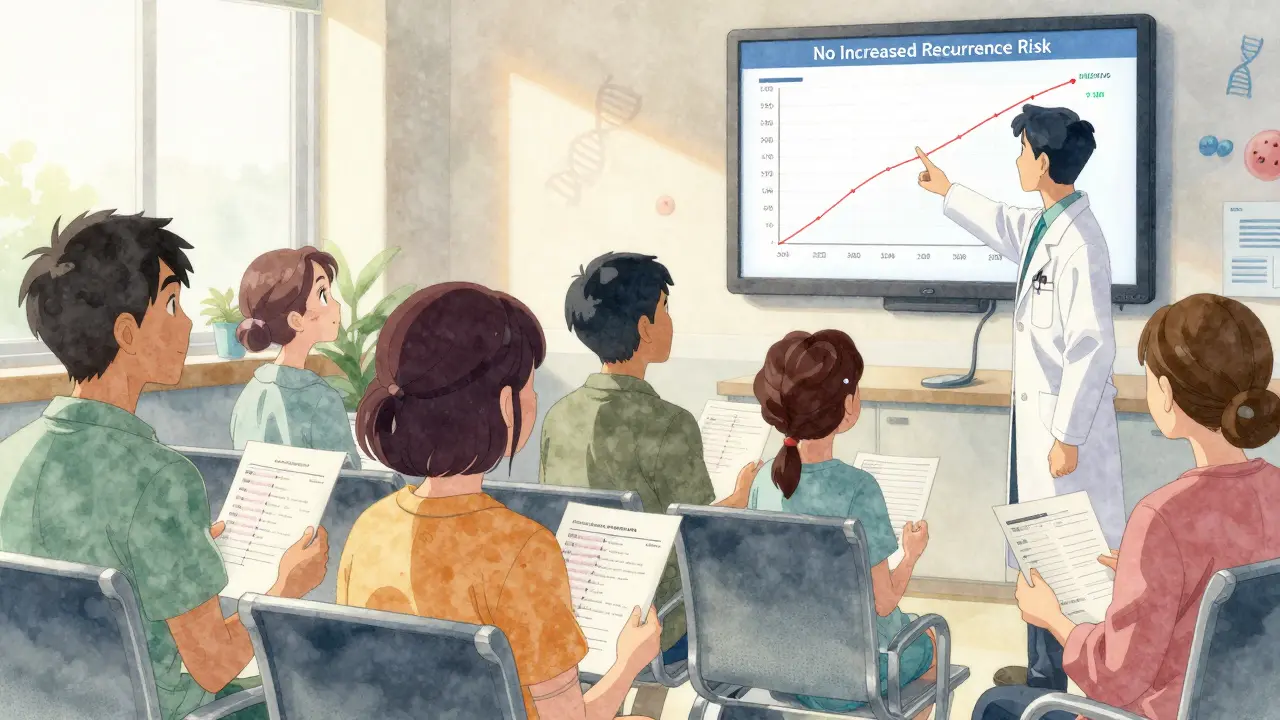
The idea that immunosuppressants cause cancer to return made sense on paper. Your immune system hunts down abnormal cells - including cancer. So if you’re taking drugs like methotrexate, azathioprine, or anti-TNF biologics (infliximab, adalimumab), you’re lowering that defense. Logic says: more suppression = higher risk. But real-world data told a different story. In 2016, a massive review of 11,702 patients with autoimmune diseases like rheumatoid arthritis, Crohn’s, or psoriasis - and a past cancer diagnosis - found no increased risk of cancer coming back, no matter which immunosuppressant they took. Not with anti-TNF drugs. Not with older pills like methotrexate. Not even with combinations of both. The numbers were clear: patients on no treatment had 37.5 recurrences per 1,000 person-years. Those on anti-TNF therapy? 33.8. Combination therapy? 54.5. That last one sounds scary - until you realize the difference wasn’t statistically meaningful. The P-value was over 0.1. That means it could easily have been random chance. By 2024, a new analysis doubled the sample size to over 24,000 patients and nearly 86,000 years of follow-up. Same result. No increased risk. Not even for newer drugs like ustekinumab, vedolizumab, or JAK inhibitors. And here’s the kicker: whether you started immunosuppressants six months after cancer treatment or six years later? It didn’t matter. The clock didn’t reset your risk.What the latest studies actually say
These aren’t small studies. They’re meta-analyses - the gold standard. They combine data from dozens of smaller trials and real-world records. The 2024 study in PMC is the most comprehensive to date. It looked at every major type of immunosuppressant used for autoimmune conditions and checked cancer recurrence rates across all cancer types. The results? No signal. No red flag. No pattern suggesting that suppressing immunity leads to more cancer coming back. Even more surprising? Some newer biologics showed a lower numerical rate of recurrence than older drugs. Not enough to call it a win statistically - but enough to make you wonder if certain drugs might even be safer than others. That’s something researchers are now digging into. The American College of Rheumatology, the European League Against Rheumatism, and the FDA all updated their guidance based on this evidence. The FDA changed drug labels in 2022 to say: “Clinical studies have not shown an increased risk of cancer recurrence in patients with prior malignancy treated with [this agent].”What about melanoma or blood cancers?
Not all cancers are the same. And not all patients are treated the same way. Experts still advise caution in two specific cases: active blood cancers (like leukemia or lymphoma) and recent melanoma. These cancers are more aggressive, and immune surveillance may play a bigger role in keeping them in check. For melanoma, in particular, some doctors still prefer to delay biologics if the cancer was diagnosed within the past year - even though the data doesn’t prove it’s risky. It’s a precaution, not a rule. For everything else - breast, colon, lung, prostate, skin cancers (non-melanoma), ovarian - the evidence is clear. No need to delay treatment. No need to avoid immunosuppressants because of your cancer history.
What does this mean for your treatment plan?
If you’re on immunosuppressants and had cancer in the past, you might have been told to stop them. Or you might have been scared to restart them. That fear? It’s outdated. Today, the goal is personalization. Your doctor shouldn’t ask: “When was your cancer?” They should ask: “What kind was it? How advanced? When did you finish treatment? How’s your autoimmune disease doing?” For example:- If you had stage I colon cancer five years ago and finished chemo with no signs of disease, restarting adalimumab for Crohn’s is safe.
- If you had aggressive lymphoma two years ago and are still in remission, your rheumatologist might wait longer - but not because of a blanket rule. It’s because your cancer’s behavior matters more than the clock.
- If your RA is causing joint damage, and you’ve been off meds for three years to avoid risk - you’re now at higher risk of disability than recurrence.
How doctors are changing their approach
Before 2016, many patients were denied life-changing treatments just because they had cancer in their past. Some went years without relief. Others switched to ineffective drugs. Some even stopped treatment entirely. Now, things are shifting. In the U.S., biologic prescriptions for patients with prior cancer histories jumped 18.7% between 2017 and 2022, according to IQVIA data. That’s not because more people are getting cancer. It’s because doctors are finally treating them based on evidence, not fear. Specialists in rheumatology, gastroenterology, and dermatology are now working together more closely. A patient with psoriasis and a history of breast cancer? They’re seen by a dermatologist, an oncologist, and a rheumatologist - all on the same page.
What’s next? Ongoing research
The science isn’t done. Two major studies are still tracking patients:- RECOVER (NCT04567821): Focusing on IBD patients with prior cancer. Results expected in mid-2026.
- RHEUM-CARE (NCT04321987): Tracking 5,000 RA patients with cancer histories to find patterns by drug type and cancer subtype.
What you should do now
If you’re living with an autoimmune disease and have a history of cancer:- Don’t assume you can’t take immunosuppressants. The old 5-year rule is gone.
- Bring your full cancer history to your doctor. Include type, stage, treatment dates, and current status.
- Ask: “What’s the risk of my autoimmune disease getting worse if I don’t treat it?” That’s often bigger than the cancer recurrence risk.
- Don’t panic over old advice. If someone tells you to wait five years, ask them to show you the study.
Monitoring after starting immunosuppressants
Even though the risk isn’t higher, you still need regular check-ups. That’s not because of the drugs - it’s because you’re a person with a cancer history. Standard screening still applies:- Annual skin checks if you’ve had melanoma or non-melanoma skin cancer.
- Colonoscopies on schedule if you’ve had colorectal cancer.
- Mammograms, Pap smears, or prostate exams based on your personal history.
- Blood tests to monitor for signs of recurrence, if your cancer type requires it.
Do immunosuppressants cause cancer to come back?
No. Large, high-quality studies involving over 24,000 patients show no increased risk of cancer recurrence from anti-TNF drugs, methotrexate, azathioprine, or newer biologics like ustekinumab and JAK inhibitors. The old belief that suppressing immunity leads to more cancer returns has been disproven by modern evidence.
Should I wait five years after cancer to start immunosuppressants?
No. The five-year waiting period was based on theory, not data. Recent studies show that starting immunosuppressants six months or six years after cancer diagnosis carries the same low risk of recurrence. Treatment decisions should be based on your cancer type, stage, and how active your autoimmune disease is - not a fixed timeline.
Are some immunosuppressants safer than others after cancer?
All major classes - anti-TNFs, conventional DMARDs, and newer biologics - show similar low recurrence rates. Some newer drugs like ustekinumab and vedolizumab showed slightly lower numerical recurrence rates, but the differences weren’t statistically significant. The choice should be based on your disease, side effect profile, and cost - not fear of cancer return.
Is it safe to use immunosuppressants after melanoma?
For most people, yes - but caution is still advised. Melanoma is more sensitive to immune surveillance, so some doctors delay treatment for at least one year after diagnosis or surgery. However, there’s no proof that biologics increase recurrence risk. The decision should be made with your oncologist, based on the stage and depth of your melanoma.
What if I’m worried about getting a new cancer?
Immunosuppressants slightly increase the risk of new skin cancers and some lymphomas - but not because of your past cancer. This is a general effect of long-term immune suppression. Regular skin checks and staying up-to-date on cancer screenings reduce this risk. The benefit of controlling your autoimmune disease usually outweighs this small increase.
Can I restart immunosuppressants if my cancer came back?
If your cancer returns, your treatment plan changes. You’ll likely pause immunosuppressants while you treat the recurrence. Once you’re in remission again, you can restart them - but only after a full discussion with your oncologist and rheumatologist. The same evidence applies: recurrence risk isn’t higher because of the drugs, but your current cancer status matters most.











