
Imagine a sharp, electric shock zipping down your arm or leg. It’s not just a twinge; it’s a burning sensation that makes you freeze in place. If this sounds familiar, you might be dealing with Radiculopathy, which is a condition where nerve roots exiting the spinal cord become compressed or irritated. While the name sounds medical and intimidating, the reality is common. About 95% of all cases happen in the neck (cervical) or lower back (lumbar). The good news? Roughly 85% of people see their symptoms go away within 12 weeks without surgery. You don’t have to live with the pain forever, but knowing exactly what is happening inside your spine is the first step to fixing it.
What Is Radiculopathy and Why Does It Hurt?
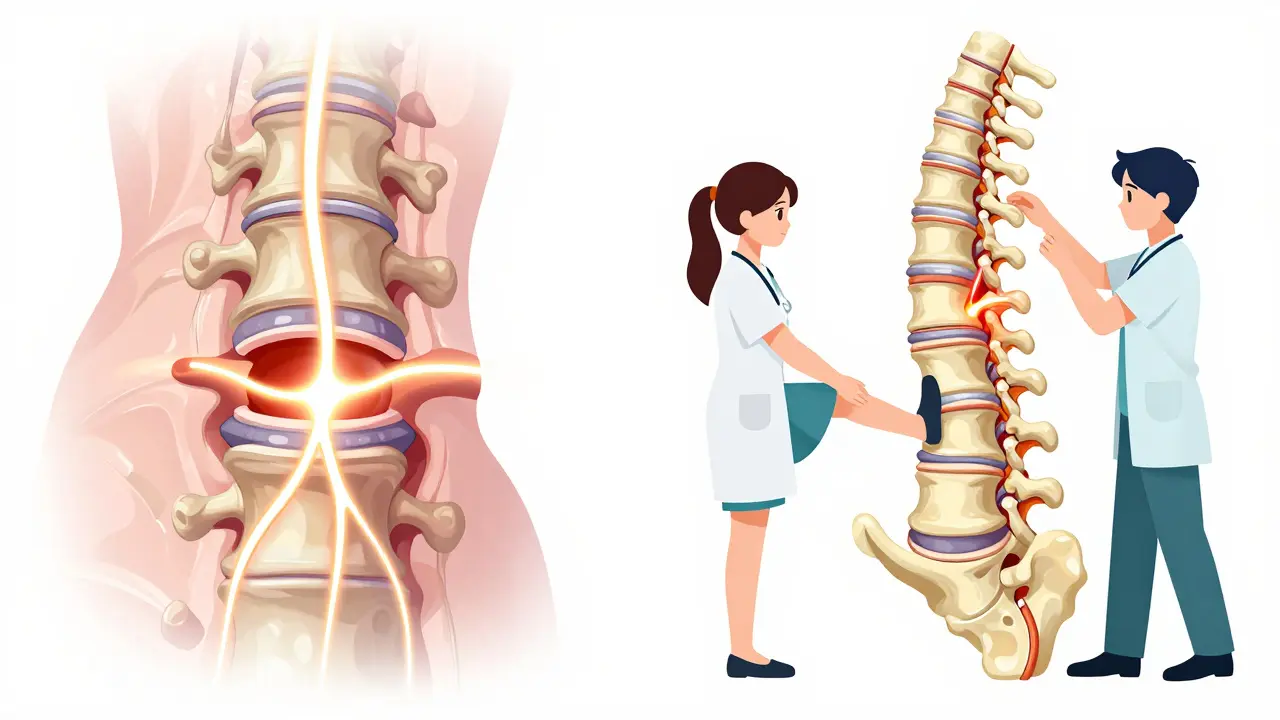
To understand why your shoulder or calf hurts when the problem is in your back, you need to look at the anatomy. Your spinal cord runs through your vertebrae, and small nerves branch off like wires from an extension cord. These are called nerve roots. When something presses on these roots-usually a disc or bone-they send false signals. This results in pain, numbness, tingling, or weakness along the specific path that nerve travels. This pattern is known as a dermatome.
The cause often depends on your age. If you are under 50, there is a 90% chance a herniated disc is the culprit. Think of a jelly-filled donut; if the soft center pushes out, it can squeeze the nearby nerve. For those over 50, wear and tear takes over. Degenerative changes like spondylosis or narrowing of the exit holes (foraminal stenosis) account for nearly 78% of cervical cases. Trauma also plays a role, with acute injuries causing about 23% of neck-related cases compared to just 12% for the lower back.
Cervical vs. Lumbar: Spotting the Difference
Knowing whether your issue is in the neck or lower back helps guide your recovery. They feel different and affect different parts of your body.
| Feature | Cervical (Neck) | Lumbar (Lower Back) |
|---|---|---|
| Most Affected Nerves | C7 (57%), C6 (27%) | L5 (49%), S1 (43%) |
| Pain Location | Shoulder, arm, thumb/middle finger | Buttock, outer calf, big toe/sole |
| Common Weakness | Biceps (C6), Triceps/Grip (C7/C8) | Foot lift (L5), Ankle push (S1) |
| Recovery Time | Average 11.1 weeks | Average 14.2 weeks |
| Conservative Success Rate | 89% within 6 months | 76% within 6 months |
If you have trouble lifting your foot (foot drop) or pushing off your toes, that points to L5 or S1 involvement in the lower back. If your grip feels weak or you can’t straighten your elbow properly, look toward the C7 or C8 nerves in the neck. MRI scans are the gold standard here, detecting cervical disc issues with 92% sensitivity, far better than older CT methods.
When to Wait and When to Act Fast
Most doctors will tell you to wait. The American College of Physicians recommends trying conservative care for 6 to 8 weeks before looking at invasive options. Why? Because inflammation often settles down on its own. However, patience has limits. You need immediate medical attention if you experience "red flag" symptoms. These include loss of bowel or bladder control, severe progressive weakness, or numbness in the saddle area (inner thighs). These could signal cauda equina syndrome, a rare but serious emergency requiring urgent surgery.
For everyone else, medication alone isn't enough. Studies show physical therapy reduces symptoms by 68%, compared to only 52% for medication alone. Many patients try epidural steroid injections hoping for a quick fix. While some report relief, evidence suggests they offer only moderate short-term pain reduction (2-6 weeks) with no long-term benefit for most people. Don't let the promise of a "quick shot" distract you from the real work: moving correctly.
Your Step-by-Step Rehab Plan
Rehabilitation isn't one-size-fits-all, but successful protocols follow a logical progression. Here is how a typical evidence-based plan looks, based on data from major clinics like Cleveland Clinic and Hospital for Special Surgery.
- Phase 1: Calm the Storm (Weeks 1-2)
Focus on activity modification. Avoid positions that spike the pain. Use NSAIDs like ibuprofen (400mg three times daily, if safe for you) to reduce inflammation. Start gentle range-of-motion movements. For neck pain, simple chin tucks help align the head. For back pain, lying on your stomach (if comfortable) can help centralize the pain away from the leg. - Phase 2: Build Stability (Weeks 2-4)
Introduce light traction or support. Cervical cases may benefit from mechanical traction (5-10 lbs) to open up nerve spaces. Lumbar cases start core stabilization. Think of exercises like bird-dogs or dead bugs that keep your spine neutral while moving limbs. The goal is to teach your muscles to hold your spine steady without straining the discs. - Phase 3: Strengthen and Load (Weeks 4-8)
Now you add resistance. Isometric strengthening comes first-tensing muscles without moving joints. Then move to dynamic stabilization. For lumbar radiculopathy, McKenzie extension exercises are key. For cervical, scapular retractions (pulling shoulder blades together) strengthen the upper back to take pressure off the neck. - Phase 4: Return to Life (Weeks 8-12+)
Functional training. Lift groceries, carry kids, or return to desk work with proper ergonomics. Data shows office workers who adjust their workstation see a 32% reduction in symptoms. Consistency is everything here. Patients who stick to home exercises recover 47% faster.
Expect to need 12 to 16 sessions of physical therapy for optimal results. Skipping sessions or doing exercises sporadically is the number one reason people fail to improve. Sixty-one percent of non-responders admitted to inconsistent performance.
Mistakes That Keep You Stuck
Even with the right diagnosis, bad habits can derail recovery. The biggest pitfall is returning to heavy lifting too soon. About 28% of symptom recurrences happen because people jump back into high-load activities before their tissues are ready. Another common error is relying solely on passive treatments. Getting massages or heat helps feel better temporarily, but it doesn't fix the mechanical compression. You must actively strengthen the supporting musculature.
Also, watch your sleep setup. For neck pain, using a pillow that supports the natural curve of your cervical spine is crucial. A flat or overly fluffy pillow can keep your nerves pinched all night. For back pain, sleeping on your side with a pillow between your knees keeps the pelvis aligned and reduces strain on the lumbar roots.
What the Future Holds for Nerve Pain
Treatment is getting smarter. New AI-assisted MRI software, approved recently, detects nerve compression with 96.7% accuracy, helping doctors pinpoint the exact problem faster. Researchers are also testing personalized exercise protocols based on which specific nerve root is involved, showing 41% greater functional improvement than standard care. While regenerative therapies like platelet-rich plasma (PRP) are gaining buzz, current evidence remains mixed, so stick to proven mechanical rehabilitation first.
Remember, radiculopathy is a mechanical problem. It requires a mechanical solution. By understanding your specific nerve involvement, following a phased rehab plan, and avoiding early heavy loading, you join the 82% of patients who return to full function within a year. Be patient, stay consistent, and trust the process.
How long does it take for radiculopathy to heal?
Most cases resolve within 12 weeks with conservative management. Cervical radiculopathy averages 11.1 weeks for recovery, while lumbar radiculopathy takes slightly longer, averaging 14.2 weeks. About 85% of patients do not require surgery.
Is cervical or lumbar radiculopathy worse?
Lumbar radiculopathy generally causes higher disability scores and longer recovery times. Patients report 37% higher disability on the Oswestry Index and take 28% longer to recover compared to cervical cases. However, cervical cases have a slightly higher success rate with conservative care (89% vs 76%).
Do epidural steroid injections cure radiculopathy?
No, they do not cure the underlying issue. Evidence shows they provide moderate short-term pain relief (2-6 weeks) but offer no significant long-term benefit compared to other conservative treatments. Physical therapy is more effective for lasting symptom reduction.
What exercises are best for nerve root compression?
For cervical radiculopathy, chin tucks and scapular retractions are highly effective. For lumbar radiculopathy, McKenzie extension exercises and core stabilization drills (like bird-dogs) are recommended. Always perform these under the guidance of a physical therapist to ensure correct form.
When should I see a doctor for back or neck pain?
See a doctor immediately if you have loss of bowel/bladder control, severe progressive weakness, or numbness in the groin area. For general pain, if it persists beyond 6-8 weeks despite home care, consult a specialist for imaging and a structured rehab plan.













