Every year, thousands of seniors end up in the hospital-not because of a fall, heart attack, or infection, but because of a medication they were told was safe. In fact, high-risk medications for seniors are one of the leading causes of preventable hospitalizations in people over 65. The good news? Many of these dangers are well-documented, avoidable, and often easy to fix with a simple conversation with a doctor or pharmacist.
What Makes a Medication High-Risk for Seniors?
It’s not about how strong the drug is. It’s about how the aging body handles it. As we get older, our kidneys and liver don’t filter drugs the same way. Muscle mass drops, body fat increases, and brain sensitivity to certain chemicals changes. A pill that’s harmless for a 40-year-old can be dangerous for a 75-year-old.
The American Geriatrics Society (AGS) keeps a list called the Beers Criteria-updated every two years-and it’s the gold standard for spotting risky prescriptions in older adults. The latest version, from May 2023, flags 30 classes of drugs and 14 individual medications that should generally be avoided. These aren’t banned. They’re flagged because the risks often outweigh the benefits.
For example, a 2022 study from the Agency for Healthcare Research and Quality found that adverse drug events cost Medicare $177.4 billion annually. Most of those events were preventable. And it’s not just one drug-it’s the combo. About 40% of seniors take five or more medications. That’s called polypharmacy, and it’s where things get dangerous.
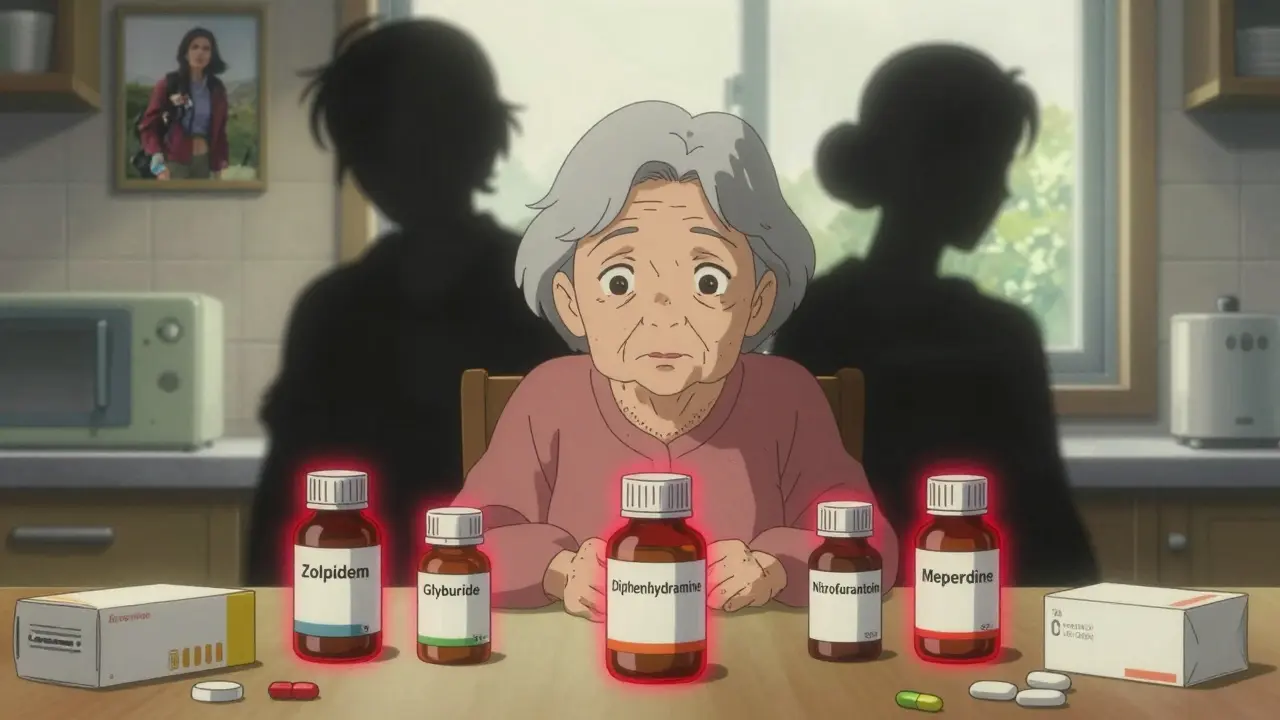
Top 5 High-Risk Medications for Seniors (and Safer Alternatives)
Here are five of the most common offenders-and what to ask your doctor instead.
1. Zolpidem (Ambien®)
This sleep aid is one of the most prescribed drugs for insomnia in seniors. But it’s also one of the most dangerous. Studies show it increases the risk of falls by 82% in people over 65. Why? The drug lingers in the body longer. Residual drowsiness can last up to 11 hours, making people unsteady the next morning. Some users even report sleepwalking or confusion.
Safer alternative: Trazodone. It’s an older antidepressant that’s been repurposed for sleep. It doesn’t cause the same level of next-day drowsiness or fall risk. Cognitive behavioral therapy for insomnia (CBT-I) is even better-no pills needed, and it works long-term.
2. Glyburide (Diabeta®)
Used to treat type 2 diabetes, glyburide is a first-generation sulfonylurea. It’s cheap. But it’s also a major cause of low blood sugar in seniors. In fact, 29.3% of older adults on glyburide have a hypoglycemic episode each year. That’s nearly three times higher than with newer options like glipizide. Severe low blood sugar can lead to confusion, seizures, or even coma.
Safer alternative: Glipizide or metformin. Both are safer for kidney function and carry far less risk of sudden drops in blood sugar. The CDC and AGS both say glyburide should be avoided in seniors unless there’s no other option.
3. Diphenhydramine (Benadryl®)
This antihistamine is everywhere-sleep aids, allergy pills, cold remedies. But it’s also a powerful anticholinergic. That means it blocks a brain chemical called acetylcholine, which is vital for memory and focus. Long-term use of diphenhydramine increases dementia risk by 54%. One study found that people who took it daily for more than three years had significantly higher rates of cognitive decline.
Safer alternative: Loratadine (Claritin®) or cetirizine (Zyrtec®). These newer antihistamines don’t cross the blood-brain barrier. They work just as well for allergies without the brain fog or memory risks.
4. Nitrofurantoin (Macrobid®)
This antibiotic is often prescribed for urinary tract infections (UTIs), which are common in older adults. But if kidney function is even slightly reduced (which it often is after 65), nitrofurantoin can cause severe lung damage. The risk of pulmonary toxicity jumps 12.8 times in people with low kidney function. Mortality from this reaction can be as high as 18%.
Safer alternative: Amoxicillin or cephalexin. These antibiotics are cleared differently and don’t build up in the lungs. Always ask for a kidney function test (eGFR) before starting any antibiotic.
5. Meperidine (Demerol®)
This painkiller used to be common after surgery. But its metabolite, normeperidine, builds up in older bodies and can trigger seizures. Studies show seniors on meperidine have over seven times the seizure risk compared to other opioids like morphine or oxycodone.
Safer alternative: Oxycodone or acetaminophen. For chronic pain, non-opioid options like physical therapy or topical lidocaine are often better long-term solutions.
How to Spot Hidden Risks in Your Meds
Many seniors don’t realize they’re on a high-risk drug because it’s been prescribed years ago-and no one’s checked since. Here’s how to take control:
- Do a brown bag review. Take all your pills-supplements, OTC meds, even empty bottles-to your pharmacist or doctor. Do this every six months.
- Check the anticholinergic burden. Look up each drug on the Anticholinergic Cognitive Burden (ACB) scale. Scores of 3 or higher (like diphenhydramine) are red flags. Total score above 3? Talk to your doctor.
- Ask: “Is this still necessary?” Many drugs are prescribed for short-term use but become long-term habits. Ask if you still need it, or if a lower dose or non-drug option works.
- Use the Beers Criteria. Search “AGS Beers Criteria 2023” online. You can download the full list. Bring it to your next appointment.
What’s Being Done to Protect Seniors?
It’s not just up to you. Health systems are starting to catch on.
Most Medicare Advantage plans now use the Beers Criteria to decide which drugs they cover. Humana, for example, limits zolpidem to a 90-day supply per year. Buckeye Health Plan doesn’t cover glyburide at all unless a doctor jumps through hoops to justify it.
Electronic health records now flag high-risk prescriptions before they’re even written. Epic and Cerner systems alert doctors in real time if they try to prescribe a Beers Criteria drug to someone over 65. Pharmacies using Surescripts’ tools have cut high-risk dispensing by nearly 20% since 2023.
In January 2024, the CMS launched a new program that ties 5% of Medicare Advantage bonuses to reducing high-risk medication use. That means doctors and insurers now have a financial reason to look out for you.
What You Can Do Today
You don’t need to wait for a doctor’s appointment. Start now:
- Make a list of every pill, patch, or liquid you take-including vitamins and herbal supplements.
- Check each one against the 2023 Beers Criteria list. Look for zolpidem, glyburide, diphenhydramine, nitrofurantoin, and meperidine.
- Write down one question for your doctor: “Could this medication be putting me at risk?”
- Ask if a pharmacist can review your meds. Many insurance plans offer free medication reviews.
- Don’t stop any drug cold turkey. Tapering off things like benzodiazepines or sleep aids needs medical supervision.
Medications aren’t the enemy. But unchecked, they can become silent threats. The goal isn’t to stop all drugs-it’s to make sure every pill you take is still the right one for your body today, not ten years ago.
Are over-the-counter meds like Benadryl really dangerous for seniors?
Yes. Even though Benadryl (diphenhydramine) is sold without a prescription, it’s one of the most dangerous drugs for older adults. It blocks acetylcholine in the brain, which can cause confusion, memory loss, and increased dementia risk. Studies show using it for more than three years raises dementia risk by 54%. Safer OTC options include loratadine (Claritin) or cetirizine (Zyrtec), which don’t affect the brain.
Why is glyburide worse than other diabetes pills for seniors?
Glyburide lasts too long in the body and can cause severe low blood sugar without warning. Seniors are more sensitive to this because their liver and kidneys don’t clear the drug as efficiently. Compared to glipizide, glyburide causes 2.1 times more hypoglycemic episodes. It can lead to falls, confusion, or even coma. Glipizide and metformin are much safer and just as effective.
Can I just stop taking a high-risk medication if I’m worried?
No. Suddenly stopping some medications-like benzodiazepines, sleep aids, or certain blood pressure pills-can cause dangerous withdrawal symptoms, seizures, or rebound conditions. Always talk to your doctor first. They can help you taper off safely, often over 4-6 weeks, and replace it with a safer option.
Do pharmacists really help with medication reviews?
Yes. Pharmacists are trained to spot dangerous drug interactions and high-risk prescriptions. Studies show pharmacist-led reviews reduce high-risk medication use by over 34% within six months. Most insurance plans offer free medication reviews-just ask. Bring all your pills, even the ones you only take sometimes.
How often should seniors review their medications?
At least once a year, but every six months is better-especially if you take five or more medications. Changes in health, kidney function, or weight can make a previously safe drug risky. Many doctors now use electronic alerts to flag high-risk prescriptions, but don’t rely on them. Take an active role. Keep a list and review it with your pharmacist regularly.















